

This study aimed to systematically review the available evidence regarding the disparity between WTA and WTP for health outcomes or healthcare goods and services.
The current state of WTA and WTP empirical research in the healthcare field
The results of empirical studies may be influenced by the selected methods of value elicitation, specifically concerning WTA and WTP questions. Among the 14 studies addressing both types of WTA and WTP questions, 8 studies revealed a significant discrepancy in response rates, with the majority (6/8, 75%) showing that the response rate for WTA questions was markedly lower than that for WTP questions.
The frequently observed phenomenon of WTA values exceeding WTP values has been consistently reported across numerous similar reviews and systematic reviews. However, this study identified that a certain proportion (6 out of 35, or 17.14%) of empirical studies in the healthcare field reported WTP values surpassing WTA values. This discrepancy may be attributed to the theoretical foundations of the CVM, the low response rates of WTA questions, the nature of public goods, and other influencing factors.
Among the six studies or subgroups reporting higher WTP values than WTA values, four did not disclose the response rates for WTA and WTP questions. In contrast, the two studies that reported response rates indicated that the rates for WTP questions were significantly higher than those for WTA questions [36], with WTP response rates being 1.69 and 4.33 times those of WTA, respectively. This low response rate for WTA questions suggests that respondents may be resistant to providing WTA estimates, potentially leading to underestimation of WTA values.
The measurement of WTA and WTP values relies on individual preference data, which inherently varies among individuals. Moreover, the distinct types of medical and health products and services described in WTA and WTP questions, along with their differing market attributes, can also influence respondents’ preferences. The declarative nature of preferences elicited by the CVM method introduces significant uncertainty into the collected results. Using monetary values to reflect preferences is influenced by various demographic characteristics, with factors such as income, education level, and personal beliefs contributing to the diversity of preferences [20, 23, 37].
Additionally, two empirical studies on the primary prevention of mother-to-child transmission of HIV, conducted by Isah in Nigeria in 2019 and 2021 [33, 36], yielded highly divergent WTA/WTP ratios of 29.19 and 0.14, respectively. This discrepancy may be influenced by factors such as response rates, sample sizes, and the characteristics of the medical and health products examined in these studies. A commonality between both studies is the significantly lower response rate for WTA questions compared to WTP questions. In the 2019 study, for instance, the response rate for WTA questions was only 4.8%, while that for WTP questions was 97.1%. The substantial disparity in sample sizes, along with the potential presence of extreme data and the uncertainty surrounding preferences, likely contributes to the elevated WTA/WTP ratio. Conversely, the significantly lower WTA value in the 2021 study may be attributed to the nature of the product itself. The primary prevention of mother-to-child transmission of HIV represents a public good in Nigeria, where the dynamics of income effects and substitution effects can lead to considerable differences, resulting in a smaller WTA value.
Reasons for the difference between WTA and WTP
Firstly, the disparity between WTA and WTP question response rates. One potential explanation is that WTP values are generally more influenced by income levels, making it easier for respondents to provide WTP estimates compared to WTA values. However, if low response rates for WTA questions are a widespread phenomenon, this raises questions about the validity of WTA data obtained in empirical studies. A related empirical study found no significant differences between individuals who provided WTA values and those who did not [19]. Nonetheless, qualitative findings suggest that individuals who did not report a WTA value likely possess an internal measure of it. The consistently low adherence to WTA questions, contrasted with high adherence to WTP questions, serves as tangible evidence of differing public perceptions regarding these evaluation methods, thereby reflecting variations in preferences.
Then, the WTA/WTP ratios differ. In various fields of empirical research, it is widely accepted that differences exist between WTP and WTA, although the underlying reasons for these discrepancies remain a topic of debate. A comparison of baseline characteristics among respondents in numerous empirical studies reveals a significant relationship between income levels and the WTA-WTP disparity [20, 21, 27, 33]. This phenomenon can be explained by the income effect in economic theory. Since WTP is constrained by income, whereas compensation claims (WTA) are not, a notable income effect emerges.
The gap between WTA and WTP may widen under certain conditions, such as when the change of concern is substantial, the value of the commodity in question is high, or when the income elasticity of that commodity is significant and increases with income [41, 42]. Specifically, as the value of goods rises, WTP increases until it reaches an income threshold, while WTA can theoretically extend indefinitely. This theoretical pattern is supported by our stratified analysis of country income levels. The median WTA/WTP ratio was highest in low-income countries, while the ratios observed in middle- and high-income countries were relatively similar, suggesting that the valuation gap is more pronounced in lower-income settings. This finding may reflect greater reluctance among individuals in resource-constrained contexts to relinquish healthcare benefits, potentially due to lower economic security, limited access to healthcare, or the heightened perceived value of health interventions.
In addition to the income effect, the substitution effect is a critical factor influencing WTA and WTP in economic theory. While WTP reflects the monetary value of an individual’s willingness to purchase a good, WTA represents the monetary value required to compensate for the rejection of that good, often interpreted as the cost of acquiring a substitute. When fewer substitutes are available, replacing the good becomes more challenging, potentially necessitating higher compensation [41]. Health, being a commodity with few or no substitutes, poses significant difficulty in assigning a monetary value to the loss of a unit of health.
Beyond income levels, other factors contributing to the disparity between WTA and WTP include measurement errors related to technology, individual cognitive preferences, and the resource endowment effect. Almost all empirical studies examining WTA and WTP employ the contingent valuation method, collecting relevant data through questionnaire surveys. The format of WTA and WTP questions can significantly influence the values obtained [43]. For instance, there can be substantial differences between the monetary willingness expressed in open-ended versus closed-ended questionnaires. Furthermore, empirical data are typically summarized using mean values; thus, the presence of extreme data points can skew results and reduce their representativeness.
The resource endowment effect, proposed by psychologists [20], serves as an explanation for observed behaviors regarding WTA and WTP. This effect is linked to loss aversion, where individuals ascribe greater value to goods they own compared to those they do not. Economically, this is expressed as a higher perceived utility for owned goods. Consequently, the compensation required for relinquishing an already owned product often exceeds the monetary value assigned to obtaining a new one, resulting in WTA values that are higher than WTP values. In the healthcare context, the monetary compensation for canceling existing medical services frequently surpasses the amount individuals are willing to pay for new services.
Economic theories explaining the endowment effect emphasize factors such as information costs, uncertainty regarding the value of goods, and the irreversibility of losses [21]. Additionally, the theory encompasses individual cognitive preferences; individuals generally prefer the products or resources they already possess. Variations in education levels and social status can further introduce cognitive biases, leading to differing degrees of disparity between WTA and WTP.
The “distortion” phenomenon of the cost-effectiveness threshold caused by the disparity between WTA and WTP
The cost-effectiveness plane serves as a geometric framework for representing incremental cost (∆C) and incremental effect (∆E) data [7]. In the plane, the horizontal axis denotes ∆E, while the vertical axis indicates ∆C, facilitating clear visualization of the incremental cost-effectiveness ratio (ICER) acceptance or rejection decision rules. The cost-effectiveness plane is divided into four decision regions, with particular attention often given to the upper-right (more effective and more costly) and lower-left (less effective and less costly) regions within pharmacoeconomic research. Points located in the upper-right region signify that a new intervention is both more effective and more costly than the existing intervention. Conversely, points in the lower-left region indicate that the new intervention is less effective and less costly than the old one. In making intervention decisions, it is essential to establish the cost-effectiveness threshold (λ). Most literature defines λ as the slope of a straight line that intersects the origin and spans the upper-right and lower-left region of the cost-effectiveness plane. This implies that the threshold remains constant across both regions, as illustrated in Fig. 2.
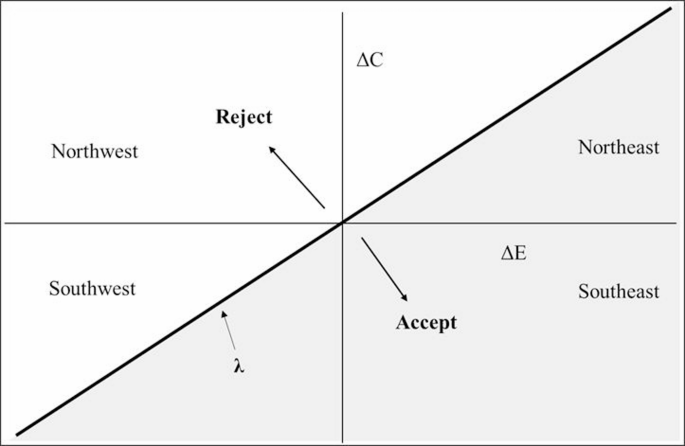
Accept area and reject area in the cost-effectiveness plane without distortion threshold
Thus, the threshold (λ) serves as a bridge to elucidate the relationship between cost-effectiveness and cost-benefit analysis, providing a mechanism for translating health effects into monetary units [7]. However, it is essential to recognize that this threshold is represented as a straight line, based on the assumption that willingness to pay for health is equivalent to willingness to accept compensation for health loss. In essence, this implies that WTA should equal WTP within the healthcare field.
Empirical evidence, however, confirms that WTA often differs from WTP, which contradicts the notion of a threshold (λ) derived solely from WTP. Consequently, O’Brien argues that cost-effectiveness thresholds in healthcare are distorted [7]. Previous empirical studies in this domain have shown that WTA values are generally higher than WTP values, with the WTA/WTP ratio exhibiting a wide range, reaching as high as 29.19 in the context of this study. Therefore, in the cost-effectiveness plane, the threshold should be represented as a curve that diverges from the origin. In this plane, the slope of the line in the upper-right region corresponds to WTP, while the slope of the line in the lower-left region represents WTA, as illustrated in Fig. 3.
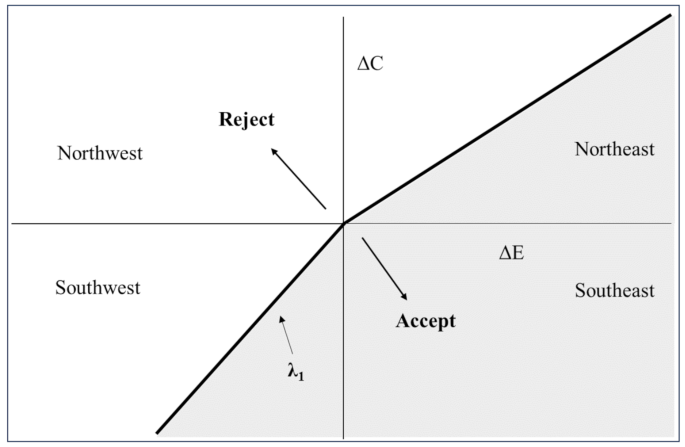
Accept area and reject area in the cost-effectiveness plane with distortion threshold
However, in the practical application of pharmacoeconomics, cost-effectiveness analyses comparing intervention programs typically yield ICER values that predominantly fall within the upper-right region [44]. This observation may explain the prevailing emphasis on the WTP threshold. If a new intervention located in the upper-right region, an ICER that remains below the WTP threshold implies that the additional cost per unit of effectiveness (e.g., per Quality-adjusted life year, QALY) is within an acceptable range for policymakers or healthcare payers, suggesting the added value justifies the higher cost [45]. Relatively speaking, if a new intervention demonstrates slightly lower effectiveness compared to an existing one while also incurs reduced costs, yielding an ICER below the threshold-WTA- in the lower-left region, which dramatically suggests that the new intervention may be deemed cost-effective. Since WTA is often higher than WTP, the area under the “kink” threshold is smaller compared to the non-kink threshold, indicating a lower probability of the new intervention being cost-effective [46]. However, healthcare policymakers often focus more on scenarios involving increased effectiveness and costs (the upper-right region), potentially overlooking the implications of cost reductions coupled with marginal decreases in effectiveness. This focus may lead to underappreciation of alternatives that, despite being less effective, offer substantial cost savings and thus warrant consideration in budget-constrained environments.
Pharmacoeconomic evaluation results are frequently utilized by healthcare administrators across various countries as a basis for decision-making. Ignoring the differences between WTP and WTA equates to disregarding the reality that decision thresholds in the upper-right and lower-left region should differ. This oversight could lead to healthcare or insurance decisions based on pharmacoeconomic evidence that are irrational, potentially resulting in societal welfare losses. Therefore, it is imperative to acknowledge and address the disparity between WTA and WTP in pharmacoeconomic evaluations.
Strengths and limitations
In this study, we employed a systematic approach to estimate the WTA/WTP ratio for health outcome or healthcare goods and services. A key aspect of our analysis involved the collection of response rates from each included study. We examined the differences in response rates between WTA and WTP questions, recognizing their significance in understanding participant engagement and the overall reliability of the data.
Our study, however, also has some limitations. We mainly present a qualitative analysis of the differences between WTA and WTP estimates without incorporating sufficient quantitative analysis. As such, it may not fully capture the comprehensive differences between the two measures. Additionally, we did not include all subgroups from two of the included articles due to an excessive number of reported values, which may introduce a slight reporting bias. However, we believe that neither of these limitations significantly influenced the overall results of the study.
link