

Study characteristics
Our search retrieved 12,332 records from the databases. After title, abstract and full-text screening (Fig. 1), we identified 69 articles that met our eligibility criteria. The included articles were from Ethiopia (n = 26), Kenya (n = 15), Tanzania (n = 9), Uganda (n = 9), Rwanda (n = 4), and other East African nations (n = 6). The studies included in this review contained relevant findings that pertained to our research question; however, there was a notable degree of variation in the depth and richness of usable information on the facilitators and barriers of HCF for universal maternal healthcare services. In the review, participants such as service users (women), men, traditional birth attendants (TBAs), religious leaders, local leaders, Health Development Armies (HDAs), healthcare providers including community health workers (CHWs) and Health Extension Workers (HEWs), maternal health coordinators, and policy personnel had participated. A total of 1,984 interviews (442 key informants, 1,186 in-depth interviews, and 356 focus group discussions) were included (Supplementary file 3).

Facilitators for maternal healthcare services
In this review, financial facilitators for universal maternal health services was one of the parent themes. The facilitators were also sub-thematized into free maternal health service policy, revenue mobilization, and risk pooling (mechanism of combining financial resources from multiple sources to share the financial risk of paying for healthcare) (Supplementary file 4). Specifically, some of financial facilitators for universal maternal healthcare services under free maternity care, risk pooling and revenue mobilization mechanisms were indicated in the figure (Fig. 2).

Financial facilitators for universal maternal healthcare services in East Africa
Free maternal healthcare service policy
In this study, 19 articles described the contribution of free maternal health policy on maternal healthcare service utilization in East Africa. The introduction of a free maternal health service policy reduces the financial burden of skilled maternal healthcare-seeking and increases service utilization [28,29,30,31]. User fee removal policy responded to the financial barriers to accessing maternal healthcare services and disregarded out-of-pocket (OOP) payments [31,32,33,34]. A woman reported that:
“Before [the introduction of] the free treatment policy for pregnant woman, many women were assisted by traditional birth attendants. This was because they were afraid of the cost involved at the level of the health facility. Some were detained at the health facility after delivery because they couldn’t pay their bills. They had to stay at health facility until they get the money but with the free treatment policy things have changed.” (Woman, FGD– Kinama, BDI) [29].
Free maternal healthcare service provision boosted skilled care utilization and improved the timing of seeking services during pregnancy and delivery [33, 35,36,37]. For example, providing free maternal services for women who complete their four ANC visits enhanced health institutional service utilization [37]. Free ANC in Tanzania enabled prenatal care service utilization [38]. Women who sought care in public health facilities acknowledged the free medical maternity services provided for all pregnant women [28, 39,40,41,42]. An interviewee service user participant suggested that:
“Many women in the community are happy about the free service. The fee for the normal delivery was 1500, and for a [caesarian section] 8000, which was really expensive, and now it is free. Compared to [a] long time [ago], many people are now coming to deliver at [the] hospital because it is free. Mothers don’t come to [the] hospital, not really due to distance, but due to the fee, whereby that fee would have helped in buying food and other things, thus one opts to deliver at home and save that money. Now many people are coming to the clinics because of the free service.” (Service user 3) [28].
Free pregnancy-related services at maternal waiting homes facilitated maternal healthcare service utilization [43,44,45]. The provision of non-medical supplies for low-income women, such as baby towels or kits, increased maternal healthcare service utilization [44]. Similarly, the provision of locally available resources, such as water, firewood, and other necessities for cooking food, to prevent their suffering from additional costs to perform their cultural ceremonies during childbirth at healthcare facilities [46]. A health extension worker reported that:
“These days, pregnant women go to the health center and stay at the maternity waiting room near term. All services are provided for free.” (20 years old, HEW) [44].
In addition, free ambulance for maternal healthcare services was helpful in improving the timeliness of referrals and women’s capacity to access health services [44]. The free ambulance service has a substantial role in minimizing a birth on the road when women travelled to the health facility [43].
Risk pooling/sharing
A total of six studies mentioned the impact of risk pooling on facilitation of universal access to maternal healthcare service delivery. Maternal and child health insurance card system assisted women to access and motivated them to deliver at healthcare facility [47]. Community-based health insurance (CBHI) is another way of a risk pooling mechanism that could help to facilitate the health-seeking behaviour of the community through reducing out- of-pocket payments [36]. A kebele leader explained that:
“The community health insurance is gaining acceptance in our village. This supports their financial needs. and governmental health facilities give maternal and child health services free. This eliminates the stress related to unplanned health care-cost expenditure.” (KII, CL#1, 30-year-old kebele leader) [36].
Government subsidizing health insurance premium load for low socioeconomic groups enabled equitable maternal healthcare services [48]. Co-payments of maternity care costs by women and the National Hospital Insurance Fund (NHIF) scheme reduced their OOPHE [30]. In Rwanda, for instance, solidarity supports poor people to utilize health services through a local scheme that can cover transport costs and exempt the annual premium for health insurance payments [49]. Affordable premium load encouraged women to save and pay for timely health insurance [50]. In Kenya, county health officials encouraged health facilities to use the NHIF to alleviate the poor reimbursement processes [30].
Revenue mobilization
Three articles explained the impact of revenue mobilization on facilitation of universal maternal healthcare service utilization. An increment in the budget for medicine and supplies for healthcare facilities improved the quality of maternal healthcare services [51]. In addition, collection of fine money (imposition of fees for women who gave childbirth at home) and putting in the health facility account assisted the health facility for another facility operations [47]. Direct disbursement of funds from the central government to the primary health facilities also reduced the long procurement process and facilitated community engagements [52].
An interviewee participant described that:
“… With this new system, health facility can procure their own needs at the right time and reduce unnecessary delays in health services provision as compared to the previous approach…”. (CHMT Level Participant, IDI) [52].
Barriers to maternal healthcare services
Barriers to universal maternal healthcare services were another parent theme. Financial barriers were further sub-thematized into direct medical costs (health spending on medical products and services used to prevent, detect, or treat a disease and its complications), direct non-medical costs (additional costs in accessing healthcare services but not directly paid for medical services. Rather it includes the costs incurred for meals, transportation, and other out-of-pocket expenses), indirect costs (the cost of productivity loss that is related to loss of income associated with the loss of working time), ineffective revenue and insurance management (Supplementary file 4). More specifically, financial barriers to universal maternal healthcare services include high health insurance premium load, delays in reimbursement, uncompensated loss of revenue, lack of healthcare autonomy, incorrect socio-economic categories, irrationality of budget disbursement, and lack of funds for mobile maternal healthcare services (Fig. 3).
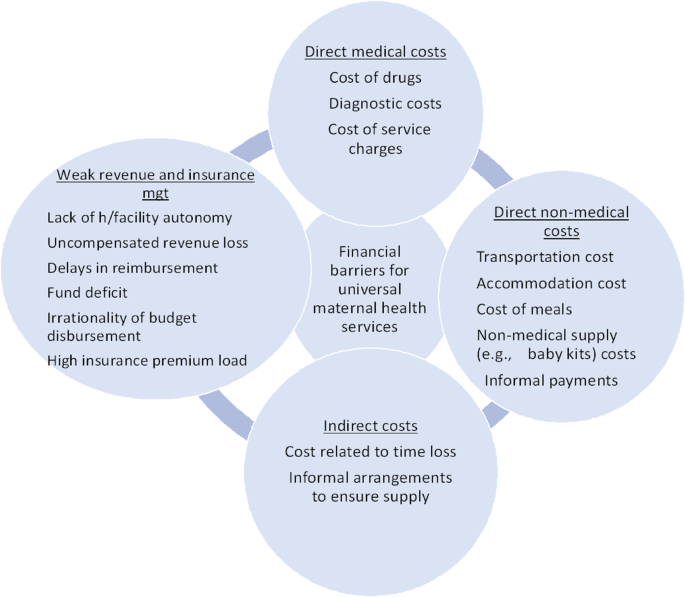
Financial barriers to universal maternal healthcare services in East Africa
Direct medical costs
A total of 39 articles described how the cost of direct medical services such as the cost of drugs, laboratory tests, ultrasound scanning, and service charges had an impact on maternal service utilization. High OOPHE and lack of money or cash to pay for maternal health costs prevented women from accessing maternal services [41, 43, 50, 53,54,55,56,57,58,59,60,61].
A 20-year-old participant reported that:
“I am financially handicapped, and I cannot afford services such as scan fees or drugs. They are surely expensive for me.” (PA 20, 20 years old) [54].
In addition, a focus-group discussion (FGD) participant commented that:
“…you are prescribed drugs to go and buy… With my meagre income I will struggle to pay for the services and sometimes one is forced to go back home with my wife without the treatment” [Partner FGD, 39–60 years Kitonyoni] [61].
Purchasing of medical supplies, the cost of emergency obstetric care including drugs, and frequent drug stock-outs from public health facilities were the critical barriers to maternal health services [35, 61,62,63,64,65,66]. Shortages and stockouts of essential medicines also influenced the quality of maternal healthcare services [67, 68]. A male traditional birth attendant (TBA) described that:
“Women who cannot afford pairs of gloves, a basin, cotton wool, one litre of kerosene, and pairs of kanga give birth at home because they do not have money to buy them.” (TBA male #2, Nyaruyeye ward) [65].
Moreover, FGD interviewee participant reported that:
“There is scarcity of ANC related medications. They were prescribed for me and I couldn’t find it in the health center, so I used to buy them from a private pharmacy monthly” [68].
Referrals to other higher-level health facilities for women with limited financial capacity increased the financial burden of specialist visits and medicines to treat their complications [51]. The costs of maternal services had a significant effect on maternal health services and forced them into financial hardship [37, 65, 69].
A male interview participant commented that:
“My wife developed pregnancy complications (postpartum hemorrhage) and it cost me a lot of money to see a Gynecology and also for transport. Many family cannot afford the cost and therefore it become an obstacle to access health services for (maternal) complications and saving mothers’ lives.” (Male participant) [51].
A midwife reported that:
“We keep them in hospital for some days until they are able to pay, some sell their possessions or exempted in case they belong to the abject poverty strata per the national wealth household categorization” (Midwife 02) [37].
A female FGD participant also suggested that:
“I spent four thousand shillings when I went to give birth. I sold the maize I had until I didn’t have food at home… Yes I sold the food to pay the hospital bills.” (FGD with women, Group 2, Participant 4) [69].
The cost of laboratory tests was expensive and significantly affected maternal service utilization [55, 65, 66].
Women delivered at home commented that:
“If you go to health facility, they ask you to get your blood, urine, stool, etc. tested for which you have to pay. Even if I have the time, I do not have the money to spend on that. I thank God I have never had any problems with my pregnancy and delivery. I delivered both my first and second children at home safely.” (Delivered at home, 27 years old) [55].
The cost of childbirth at private hospitals was found to change women’s decisions on their place of delivery [32, 39, 64]. Financial insecurity prevented women from seeking care at private health facilities and those participants who had prior experience delivering at private facilities switched to public facilities for subsequent births due to the high cost of private healthcare facilities [67]. A 34-years-old IDI mother reported that:
“The delivery service in the health facilities is of poor quality. Most of the deliveries in the health facilities are attended by students. The students give priority to their learning than to the welfare of the mother and the baby. A woman whose delivery is attended by a senior gynecologist is a lucky person because it is too difficult to get them, particularly in the government health facilities. However, the senior professionals are available in the private clinics but the cost of delivery service in the private clinics is too much. Due to this fact, women who can pay will go to private clinics and get quality service while women who are unable to afford the cost are obliged to give birth at home.” [32].
A woman in FGD described that:
“In private hospitals, the service is great but the cost is too high. For example, for those who go to deliver at [a private] hospital in Dar es Salaam, the service is superb but not everyone can afford it.” (FGD, Woman 4) [64].
Non-application of free maternity services at private hospitals enforced women to cover all costs associated with their maternity services [70]. Purchasing expensive drugs from private drug stores exerted an extra economic burden on women and their families and it did not allow many women to seek care from emergency obstetric and newborn care [36, 71]. For example, homeless mothers encountered financial constraints to purchase maternity services that are unavailable at public health facilities [72]. In healthcare facilities, prescribing medicines to be bought from private pharmacies was a common practice during maternal healthcare service delivery [55, 73]. The cost of medicines and diagnostic services (e.g., laboratory and ultrasound) from private health facilities or pharmacies were expensive and unaffordable for poor mothers for purchasing the health services [55, 74].
Free maternity services were never truly/entirely free, and some public facilities continued charging for maternity services [75, 76]. As such, some public hospitals requested payments against the free maternal health service policy that could hinder early referrals to high-level care and expose them to delayed care [44, 73, 77]. For example, poor women who have low bargaining power experienced out-of-pocket (OOP) payment for laboratory services and medicines to get essential maternity services in public health facilities [75]. For example, a male FGD participant described that:
“I took a mother to a health facility for delivery and paid for intravenous fluid and drugs while the delivery service is free of charge.” [73].
While another HEW reported that:
“…the government stated [has a policy] maternal health services are to be provided free of charge, but women pay at hospital for delivery services, so I [HEW] stopped referring mothers to this hospital.” (HEW, FGD) [77].
In another study population, a female FGD participant explained that:
“What I dislike about the hospital is that after delivery, the mother is asked to pay money, but we don’t have money; we just go there to get help.” (Female FGD participant, Meen village) [78].
Similarly, a service user replied that:
‘’The free services [are] good but there are no drugs and laboratory reagents to do the ANC [antenatal care] profile, thus we are told to go to another facility for lab work. I can’t say [the] free service will help me or not help me.” (Service user 12) [28].
Healthcare facilities faced difficulties in providing free maternal services associated with war-related healthcare destruction and looting of medicines [79]. For example, a 35-years old male manager in war affected area explained that:
“Maternal and child health services are free although the guideline states that free services will be reimbursed by the regional council but not implemented. It was only covered by the hospital and the hospital has been selling medicines to other patients and making money. It was not difficult to provide free maternal services before. But now the medicine has been stolen, the immovable has been destroyed from here. So now it is very difficult to provide free services. Because the amount of money you collect on credit is very small.” [79].
Provision of inequitable maternal healthcare service between payable and free maternal health service users affected maternal service delivery. For example, women who were able to pay for needed tests and medication services received more timely care than their counterparts [80].
Direct non-medical costs
A total of 46 articles described the impact of direct non-medical costs on maternal health service utilization. These direct non-medical costs include the cost of transportation, accommodation, food, non-medical supplies, and informal payments for healthcare providers. The cost of accommodation for women and their families accompanying the woman to a health facility affects health facility delivery [35, 47, 58, 70, 73, 76, 77]. Fear of the unaffordable cost of food for a family accompanying a health facility was also another challenge for health service uptakes [35, 36, 41, 43, 47, 58, 70, 73, 77, 81, 82]. A key informant reported that:
“If the husband does not have enough money, his wife would become hungry because she needs food after giving birth. The women who come from rural areas often do not have money to cover their costs.” [73].
Similarly, Batwa participants described that:
“what can stop me going to antenatal care is when I don’t have money to pay”, and “when we go to the hospital, the hospital needs money, yet we don’t have money. We don’t have food to eat at the hospital. That’s why we decide to stay home.” [58].
Accumulation of adequate capital to cover the costs associated with their stay at the health facility was difficult for women and this pushed them to deliver at home [47]. An inability to afford to fulfill the required delivery items associated with poverty has a negative influence on the healthcare-seeking behaviour and utilization of maternal healthcare services [42, 50, 58, 65, 83]. For instance, pregnant women are expected to provide certain materials such as basins, soap, blankets, maternal dressings, and newborn items for giving birth at the health centers as part of the ANC program and this can be a barrier to attending ANC for those with a lack of financial resources [42].
Out-of-pocket costs for transportation precluded women from maternal health service utilisation [31, 32, 36, 38, 41, 42, 47, 50, 51, 53, 54, 56,57,58,59,60,61,62,63, 65,66,67, 70,71,72,73,74, 76, 77, 81,82,83,84,85,86,87,88,89,90,91]. Fear of the unaffordability of transportation costs during emergency obstetric and newborn care was mentioned as a barrier to service utilization [36]. The cost of transportation worsened the financial burden among women at health facilities and during their referral to a higher health facility [38, 51, 67]. Fear of high cost of transportation back to their homes were the critical issues for women to attend health facility delivery [41, 62, 76, 87]. For example, if women become critically ill and felt they were going to die, they would not take them to the facility for fear of the cost of transport back to their homes [41]. Transportation fees were the predominant barriers women identified to adhere ANC attendance as per recommendations [42, 54, 58, 82, 83, 86]. In one study a community leader explained that:
“The other problem is the ambulance which does not provide round trip service and we have no other means of transportation to get back home. This is a big challenge for us. Especially some community members do not take critically ill women (pregnant or laboring) to the health facility, because if she dies at the health center or hospital returning the dead body will be too expensive, about 3,000–4,000 birr —[equivalent to USD 102–136].” (Community leader, FGD) [41].
While in another study a 32-year woman commented that:
“Transportation cost is expensive, it could be more to going back home after delivery, and we cannot afford that, therefore we prefer to stay home” (FGD women participants,32 years) [62].
Furthermore, a midwife suggested that:
“For example, the hospital have been providing adequate ambulance services but clients need to cover 80ETB (~ 3USD) for a single trip ambulance service” (h3p1) [70].
Fuel was not available or not enough in most health facilities. So, mothers were required to pay for fuel to the ambulance, but economic constraints to cover the cost of ambulance fuel was also a critical challenge to using maternal health services, particularly for women who use institutional delivery services [57, 71, 73, 77, 91]. In some cases, women are also required to cover both ambulance fuel and drivers per diem [71]. Married female FGD participant described that:
“Their husbands would be asked to cover the fuel cost of the ambulance service, which may not be affordable. Hence, women prefer to give birth at home.” (Female FGD participants) [73].
While an interviewee participant explained that:
“…we have transport [ambulance], but it has its challenges too. We don’t have enough fuel…., so patients are supposed to pay for fuel. They don’t like it, but what else can we do, they feel like we are denying them their rights.” (Participant 7) [91].
Bribery and informal payments to health workers contributed to unsupportive and negative experiences at the health facility [30, 39, 59, 67, 92, 93]. For example, casual and theatre staff experienced financial exploitative practices. As such, they asked for money from women using outdated payment rates without providing receipts [30]. Women were also discouraged from attending ANC because of being asked by the health facility staff to pay money [93]. In Uganda, bribes or informal payments to health workers were a common practice and health workers might be refused to provide care unless they paid them [67]. One woman from Rubaga division reported that:
“…in order to treat you well you have to pay them [health provider] some money… to pay attention to you… [so] I gave them 60,000 Uganda shillings.” [67].
Another participant from a public health facility stated:
“… they attend to you well if you have bribed them. They don’t spend more than 3 minutes away before coming to find out how you are doing. When I got to the labour ward there were women who were being treated better and we were wondering why, until later we came to find out that they had given the health workers money.” (Respondent #60, Public health facility) [92].
Indirect costs
Nine articles explained the impact of indirect costs on maternal healthcare service utilization. Productivity loss associated with time lost during healthcare visits was the barrier to maternal healthcare utilization [48, 66, 72, 81, 82, 84]. For instance, agricultural and household activity loss during service utilization [84]. Mothers also reported that leaving their children, cattle, and plowing land alone was another critical challenge to maternal health service uptake [81]. An example came from an interviewee FGD participant who said:
“…even if he [husband] told me to go there [health facility] I did not do that because he cann’t cover all the agricultural activity.” (FGD participant) [84].
In another study, a homeless woman shared her experience:
“…I spend my time caring for my children and in begging practices; my life is hand-to-mouth. Therefore, though I know the presence of a healthcare facility, I do not have time to go there. I have three children, so how could I go to the healthcare facilities leaving them alone without food?” (HW04: a homeless woman) [72].
An informal arrangement to ensure the availability of drugs and supplies and payment for poor mothers by healthcare providers resulted in mistrust, inequities, and negative experiences among mothers who could not afford the extra costs [30, 94]. Deliberate failing of healthcare workers on building of rapport, having rude behaviour, and mistreatment of women affected their attitude towards free maternal healthcare service utilization [95].
Ineffective revenue and insurance management
Eleven articles explained the impact of ineffective revenue and insurance management on universal access to maternal healthcare services. Delays in reimbursement to the OOPHE for prescribed drugs by health insurance were a drawback for maternal healthcare services [41]. The cost of health insurance was also a challenge to use healthcare facilities for poor households and households with large families, who had to buy health insurance for all the family members [48]. In addition, women who had national hospital insurance funds were forced to pay for drugs, diapers, soap, and buckets and co-pay for more expensive services such as ambulance service during referrals to secondary maternity health facilities [39]. Incorrect categorization of socio-economic groups could negatively affect women’s eligibility for government support for health insurance [48]. Inadequate reimbursements from the NHIF were a constraint for maternal healthcare services and exposed many patients to medical costs outside the facility [31]. Insurance premiums paid by members of the public were insufficient to cover the cost of services, which put those without health insurance under pressure [49]. A nurse explained that:
“There is a limit to which the cost of services can be covered by the revenues from health insurance premiums. For a delivery, for instance, we use up to ten pairs of gloves; beyond that, the health insurance doesn’t cover the cost.” (FGD with nurses, Rwamagana district) [49].
Contradictions between the government’s promise to provide universally free perinatal health care due to the lack of resources associated with corruption required for perinatal care [96]. Delays and failure of the national Government to reimburse funds were the challenges to the shortage of supplies and quality of maternal healthcare [33]. Duplication of payments for delivery services by the Ministry of Health (MoH) and national hospital insurance fund was another challenge in fund management for mothers [31]. Uncompensated loss of revenue for healthcare facilities providing free maternal healthcare services can be a source of frustration for administrators in sustaining the continuity of health services [33]. In addition, lack of autonomy affected public healthcare facilities’ ability to access funds and procure necessary hardware, hire staff to lodge claims, and purchase essential supplies, enabling them to generate more revenue to improve the quality of care [31]. The lack of computers, unreliable internet connectivity, insufficient medical equipment, and inconsistent stock availability from the Medical Stores Department have made it increasingly challenging to obtain missing items from the designated prime vendor in the implementation of the direct health facility financing program in Tanzania [52]. A facility in charge reported that:
“…We don’t have a computer and it’s supporting accessories to run this system. This wastes us time and finances to travel to Pangani hospital to produce a voucher, in addition we faced unnecessary delays to process facility requirements due to poor internet connectivity to run this system… ” (Facility in charge, IDI) [52].
Unpredictability, irregularity, irrationality, and unrelated budget disbursement with the number of deliveries both at health facilities and counties were the critical barriers to the provision of maternal health service [30]. Funding deficits and human resources were the major challenges to providing mobile clinic services for pastoral communities [97]. In remote settings, scarce financial support to health workers per diem payments from the district authority seemed to hinder health workers’ efforts to provide ANC and PNC outreach services [91]. A key informant participant suggested that:
“…Mobile and outreach services are very expensive. I cannot provide you with exact costs in numbers, but these services are expensive because of many factors. You must pay for the car and maintain it; you also have to take into account the costs of supplies and awareness campaigns…” (Clinician, KI #15) [97].
link