

Literature search
Full details of the literature search results are reported in Fig. 1. Forty-four TPPs were deemed eligible for inclusion in the systematic review [8,9,10, 21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61]. Inter-reviewer agreement was high at title and abstract (κ = 96%) and full-text screening (κ = 98%). For more details, please see Additional file 3: Table 3.1 and 3.2.
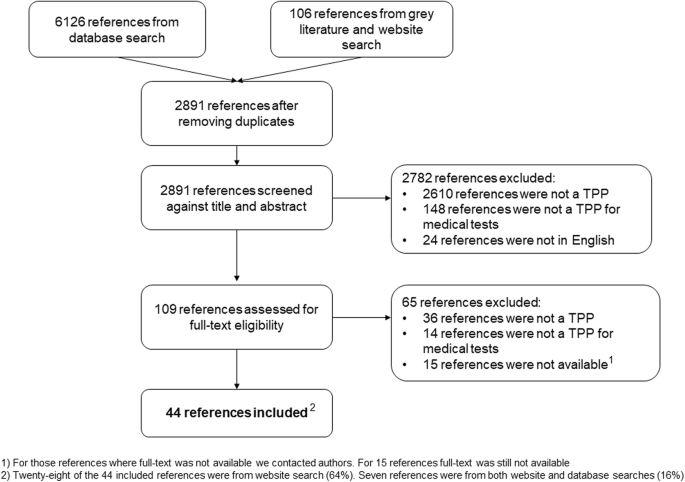
PRISMA flow diagram illustrating literature search results
Features of included TPPs
The included 44 TPPs consisted of 23 reports, 16 journal articles, 4 published TPP tables (a TPP without any background information or context e.g. [34]) and one conference poster. All TPPs provided guidance on developing medical tests to detect infectious diseases. Fourteen of the 44 TPPs focused on neglected tropical diseases (32%) (e.g. soil-transmitted helminths, Chagas disease, human African trypanosomiasis, schistosomiasis, trachoma, taeniasis cysticercisosis) and on tests for vector-borne infections (32%) (e.g. Zika virus, dengue fever, hepatitis C, malaria, E. coli). Other types of infection included sexually transmitted infections (16%, n = 7), respiratory infections (14%, n = 6) (e.g. lower respiratory tract infection, tuberculosis, pneumonia), Ebola virus [57], meningitis [61] and severe febrile illness [8].
Seven of the 44 TPPs were funded by Bill and Melinda Gates Foundation (16%), and three TPPs received funding from WHO [8, 48, 49]. The healthcare setting of interest was mostly low- and middle-income countries. The majority of TPPs did not disclose funding sources (64%, n = 28).
In some TPPs, a time horizon was chosen to represent the timeframe within which achieving the specifications described in the TPP was considered feasible [22, 23, 60]. In one TPP, this was based on a landscape analysis [22]. In another, expected advancements in technologies and knowledge related to a certain field seemed to justify the time horizon considered for the TPP [27]. Of the 44 TPPs identified, 7 reported the time horizon during which the information included in the TPP will be relevant for manufacturers (16%). Of these, 6 TPPs stated a time horizon of 5 years [22, 23, 27, 28, 51, 60], whilst the remaining considered a time horizon of 10 years [29].
Decision-making steps
A common decision-making framework, consisting of three distinct phases, was apparent across the included TPPs: scoping, drafting and consensus-building. Figure 2 presents the most commonly adopted activities, input sources and engaged stakeholder groups.

Typical activities involved, input sources and stakeholders invited for each decision-making phase
Table 1 provides a summary of the stakeholders contributing to each phase. Some of the included TPPs are not included in Table 1 as they did not report any information related to input sources or stakeholder groups [33,34,35,36, 52, 53, 55, 61]. A summary of the input sources reported to have been used at scoping and drafting phase can be found in Additional file 3: Table 3.3.
We will therefore describe the aim of each phase and breakdown the methodology (activities, input sources and stakeholders) used within the included TPPs where reported. For specific details on each included TPP, see Additional file 3: Table 3.4.
Scoping phase methodology
Half of the TPPs provided some information on the scoping phase (n = 22). The aim of this phase was to provide an overview of the disease area and the limitations associated with existing technologies. The clinical problems and unmet needs were defined, in addition to identification of which test characteristics to include in the TPP.
Some of the key activities undertaken during the scoping phase included reviewing published literature (n = 6) or available data (n = 1), and introductory meetings with stakeholders (n = 4).
Some authors reported (n = 4) [22, 26, 37, 50] that they had conducted a ‘landscape analysis’, providing information on the disease area of interest, available diagnostic technologies and related characteristics and limitations. These were usually based on interviews with stakeholders and reviews of the literature. Only Toskin et al. [50] conducted a systematic literature review, reporting the databases searched and key words used.
Consultation with experts (68%, n = 15) and the literature (36%, n = 8) were the most commonly sought sources of information during the scoping phase (see Additional file 3: Table 3.3. for a full breakdown). Only one type of source was considered in 15 TPPs (of which 11 was consulting experts), whilst 7 TPPs considered more than one source.
Denkinger et al. [22] mapped the diagnostic ecosystem of interest and then performed a survey to gauge stakeholders’ preferences. Reipold et al. [48] identified the main characteristic categories (e.g. scope, performance, operational characteristics and pricing) to be included in the TPP.
Five TPPs involved a priority-setting exercise which entailed ranking each identified health need [23, 28, 32, 48, 60].
During the scoping phase, a variety of stakeholders were engaged (Table 1).
Drafting phase methodology
The first draft of each TPP was usually prepared by either an established working group comprising experts from different organisations [9, 26, 29, 32, 40, 50, 58] or authors of the published TPP. There were two cases where the TPP was drafted by a completely different organisation [51, 57]. The TPP was often revised several times, and in some cases, it was then shortened to ensure it could be easily communicated to different stakeholders [22, 23, 28, 29, 60].
Of the 44 included TPPs, 33 of them reported which input sources were considered during the drafting phase (75%) (Additional file 3: Table 3.3). Common input sources for populating test characteristics were expert consultations (n = 22) and reviews of the literature (n = 22). Some also referred to mathematical models (n = 9), available data (n = 7), guidelines (n = 6) and ‘field observations’ (n = 5). Only one TPP was informed by pooled data from a systematic review [50].
Twenty-six of the 44 TPPs took into consideration more than one type of source at the drafting phase, as opposed to 7 TPPs which only adopted one (Additional file 3: Table 3.3). Meeting inputs were the most common single source (43%, n = 3).
The stakeholders engaged in the drafting phase are reported in Table 1.
Consensus-building phase methodology
Initial agreement with the TPP was often obtained using a survey of the stakeholders (n = 14). The survey either included general questions regarding stakeholders views on the TPP (n = 4) [22, 25, 27, 51] or adopted a Delphi-like approach to provide an initial consensus on various aspects of the TPP (n = 10). A consensus meeting with stakeholders and experts was typically held (n = 11) and a revised TPP generally agreed upon. In some cases, an additional survey was sent to stakeholders on trade-offs between test attributes [48], or on rating key parameters [51, 53]. For 2 TPPs, the final TPP draft was presented to a broader stakeholder base to validate it.
The number of participants invited to the consensus-building meetings varied (< 20 participants: n = 5; between 20 and 50 participants: n = 7). One meeting included 100 participants [27]. For a few of the TPPs, the authors also took part in the consensus meetings [29, 38, 58, 60].
Less than half of the included TPPs reported information on the activities and stakeholders invited to the consensus-building phase (n = 19). The stakeholders engaged in the consensus-building phase are reported in Table 1.
Transparency in reporting methods
We also assessed the transparency of the TPPs in terms of reporting their methodology (see Additional file 3: Table 3.5). The decision-making process behind the TPP was not reported in over a quarter of the included TPPs (n = 16). Further to this, many failed to report which information sources were considered to populate the TPP (n = 11). Just under half did not report which stakeholders were involved in the development of the TPP (n = 20). Specifically, the name of the organisations stakeholders were part was only reported in 11 TPPs, whilst 9 TPPs mentioned personal details of each stakeholder (20%) and 4 TPPs explained why certain stakeholders were invited [26, 38, 46, 58]. Sixteen TPPs reported the source of funding (36%).
There were some TPPs where the methodology was very clearly reported [26, 28, 38, 60].
Test characteristics included in TPPs
After removing duplicates, 140 different test characteristics were reported across the included TPPs. Some features which did not represent test characteristics have been excluded, such as factors relating specifically to the disease in question rather than the test. For more information, please see Test Characteristics Overview Excel spreadsheet (Availability of data and materials). Figure 3 shows the test characteristics most frequently reported (a full list is available in Additional file 2: Table 2.1).

Test characteristics frequently reported in all TPPs (n = 44) sorted by categories
Figure 4 depicts which characteristic categories were reported in the included TPPs. Details on unmet clinical need, analytical performance and clinical validity appeared to be consistently reported; however, regulatory requirements, environmental footprint and clinical utility were less frequently considered.

Test characteristic categories in absolute number (n) of included TPPs
link